
An extra dimension
Cone beam computed tomography is a powerful tool Endodontists can use to aid their treatment planning and execution. The three dimension view of the tooth reveals any missed anatomy, position of fractured instruments and perforations and is extremely useful when planning surgical treatment. In this case the preoperative periapical radiograph suggests there was a missed canal and a CBCT scan proved to be helpful in the overall treatment.

This pre-op radiograph shows a root filled LR5 with an apical radiolucency and a radiolucent line running down the centre of the root.
The initial root treatment was completed over four years ago and based on the ESE guidelines from 2006, an apical radiolucency which persists after four is considered to be associated with post treatment disease, unless healing is by scar tissue. Based on this root canal retreatment is indicated for the LR5. Furthermore, the radiolucent line in the middle of the canal needs to be investigated further to determine whether it is a missed canal or a groove on the external root surface.

CBCT scan revealing the missed canal.
Knowing where the missed canal is in three dimensions (its bucco-lingual, mesio-distal and depth position) helped me locate its entrance after removal of the existing root filling material.
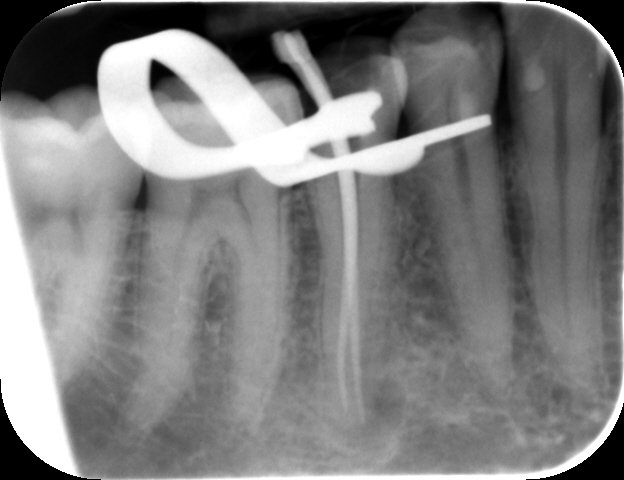
Intra-operative periapical radiograph confirming preparation of the missed canal to a good length.
Obturation was completed with gutta percha and AH plus using a warm condensation technique. The patient is now ready to return to his GDP to have the crown made and protect the tooth from future fractures. In this case the CBCT scan was invaluable in diagnosing the failure of the initial treatment and also in carrying out the treatment.
The GDP who referred this patient was planning to crown the LR5 after part of the tooth broke away. A periapical radiograph was taken to assess the tooth for the crown and an apical radiolucency was discovered. The patient has had no symptoms from this tooth since the original root canal treatment was completed and the question from the GDP was; is it ok to continue with the crown?

This CBCT view shows the DO restoration in the crown of the LR5.
After discussion with the patient we decided that taking a CBCT scan will reveal the true nature of the radiolucency in the LR5. As the view continues more apically it is clear that there is a missed canal and that it is positioned mesio-buccally to the filled canal. This valuable information aids the treatment plan and therefore the treatment itself.

Further apically more pathology and anatomy can be seen, the apical radiolucency and the mental foramen.
The working lengths for both canals were confirmed using an electronic apex locator and after preparation the lengths were confirmed with a master apical cone radiograph.

Post-op periapical radiograph shows well condensed obturation.